

Communication, whether public or private, plays a significant role in contributing to stigma (Escandon, 2024). In particular, the media and social media strongly influence community beliefs, knowledge, and attitudes towards mental health issues, suicide, and alcohol and other drug (AOD) use (Ross et al., 2019). In fact, language is a life-or-death matter; media and social media depictions of suicide can increase the risk of further suicidal behaviours and deaths (Niederkrotenthaler et al., 2020).
Even though there’s plenty of evidence showing that language matters, there still seems to be no clear agreement on what terms we should be using. For example, in a blog published by Huggett in 2020 researchers found that when people with lived experience of suicide were surveyed, their opinions were surprisingly mixed on the phrase ‘committed suicide’ – a phrase often perceived as outdated and stigmatising. On top of that, while there are several guidelines out there for how mental health should be talked about in public spaces like the media (e.g. Mindframe guidelines) or on social media (e.g. #chatsafe – see Catchpole, 2020), there’s very little advice on what language to use in personal conversations to help reduce stigma.
The aim of a recent Australian study by Elizabeth Paton and colleagues from Everymind in Australia (2024) was therefore “to develop evidence-informed guidelines for a national audience, beyond media and public communicators, that highlight how language selection in personal or public communication can be used to reduce stigma, connect communities, reduce harm and encourage help seeking and offering behaviours.”

Language matters when it comes to mental health, but what language should we be using to reduce stigma?
Methods
A mixed methods approach was used that incorporated i) focus groups ii) a delphi consensus survey and iii) an evaluation survey. The project was shaped by people with lived experience.
Focus groups were held with professional communicators, people with professional or personal experience of mental health issues and people identifying as, or working with, priority populations (e.g. young people, Aboriginal and Torres Strait Islanders). In total, 49 adults residing in Australia took part in a focus group. Focus groups were transcribed verbatim and analysed using reflexive thematic analysis.
The themes created from the focus groups were then used to develop a survey to be used in a Delphi technique. Participants (Australian adults that either had professional experience in media or other communication roles OR professional experience in the mental health sector OR personal experience of mental health issues) were asked to rank a set of statements according to their importance for inclusion in a set of guidelines. A second survey was completed to re-rate items that either didn’t reach consensus or where some confusion over the item was indicated in open ended responses.
The guidelines were launched in April 2023 via a webinar, and 60 participants completed a survey to evaluate the uptake, use, usefulness and distribution of the guidelines. Website analytics were also collected to monitor downloads.
Results
Focus groups
Participants viewed the story and narrative as inseparable from word or image choices though it was acknowledged that words can help shift the narrative towards more hopeful, recovery-oriented storytelling. Participants felt there was no ‘one size fits all’ approach to safe, inclusive representations and that diverse populations should be better reflected in public stories. Participants felt that language should be tailored to each context and informed by those affected to avoid making assumptions. There was a preference for language that moved away from clinical labels and focused more on health and wellbeing. Participants wanted more balanced, strengths-based and hopeful public representations of mental health that reflected individuals unique, personal experiences.
Delphi survey
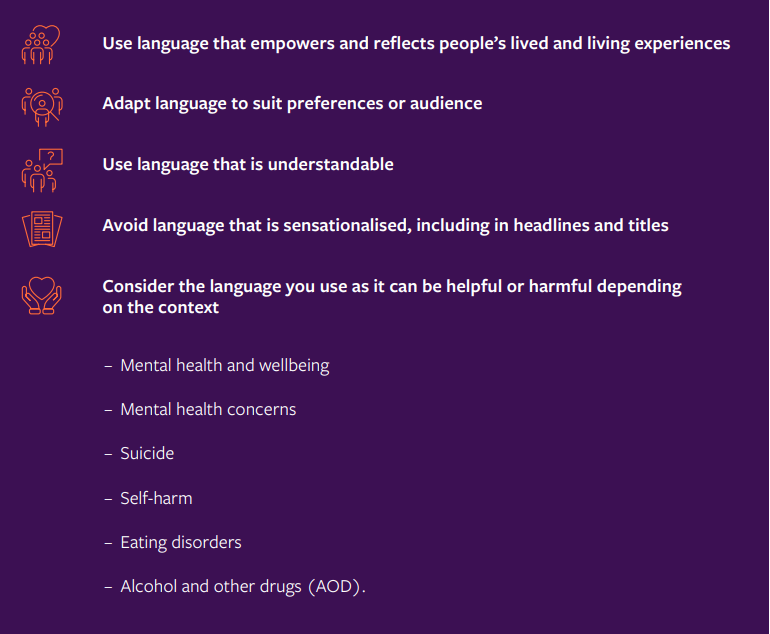
A total of 36 (out of 43 possible) statements achieved consensus across both rounds of the survey and were included in the development of the language guidelines. The key messages of the guidelines were:
- Use language that empowers and reflects people’s lived and living experiences
- Adapt language to suit preferences or audience
- Use language that is understandable
- Avoid language that is sensationalised, including in headlines and titles
- Consider the language you use as it can be helpful or harmful depending on the context.
Evaluation
Eighty-five percent of participants had viewed or downloaded the Our Words Matter resources since the launch event. Participants had mainly applied the resources to work in clinical settings and training and facilitation. Around two thirds of respondents had recommended or shared the resources, primarily with other service providers. Nearly all respondents (97.3%) agreed that the guidelines for language use were useful and stated they would continue to use these. The ‘language card: suicide’ received the most downloads (297 downloads), followed by ‘language card: mental health concerns’ (230 downloads) and ‘quick reference guide: service providers’ (183 downloads). The guidelines themselves were downloaded 59 times in the evaluation period, and read 1,284 times via Issuu (a digital reader platform embedded in the website).
There is no ‘one size fits all’ approach to safe and inclusive language; we need representations that accurately reflect the individual and unique experience of mental health, suicide and use of alcohol and other drugs.
Conclusions
The authors conclude that:
At the commencement of the project, researchers identified a gap in existing guidelines, policy and literature to support communication of mental health concerns, suicide, and AOD [alcohol and other drug] use. This gap in evidence can contribute to inaccurate, misleading, and stigma-laden language which is counterproductive to the identification, prevention, treatment and recovery of mental ill health, suicidal distress, suicide bereavement and AOD use challenges in people’s lives.

This study fills an important gap that will contribute to reduction of inaccurate, misleading and stigma-laden language.
Strengths and limitations
The authors should be commended for their inclusion of lived experience researchers in this project, particularly in seeking opinions on the direction of the project at the very start; a stage of the research cycle that seldom involves those with lived experience. The mixed methods approach used in this study helps to capture both the nuance as well as the broad, top-level insights – both of these things are needed to inform policy. It was also nice to see a real-world lens applied to this study – evaluating how the guidelines are actually being used in the ‘real world’ was a great complement to the more scientific development of the guidelines.
For me, the main limitation of this study is its scope. The authors claim in the introduction that they intend to “develop evidence-informed guidelines for a national audience, beyond media and public communicators, that highlight how language selection in personal or public communication can be used to reduce stigma, connect communities, reduce harm and encourage help seeking and offering behaviours”. I’m uncertain whether the perspectives of 45 predominantly White Australian females and an additional 30-60 survey respondents (with no specified demographics or exact number) are sufficient to address the broad scope of this work, particularly given the national audience and the three huge areas it aims to cover: mental health, suicide, and alcohol and other drugs (AOD). The sample does not seem sufficient in size, or diversity, to be able to draw conclusions and implications about language for the 26.6 million people living in Australia today. The authors speak in the discussion section about the gaps in the literature that this study has filled, but do not describe any sort of systematic approach to searching the literature to begin with. I do wonder if there is merit in such an activity, which may have added weight to the focus group findings and provided a wider pool of statements to be used in the Delphi process.

This study aimed to bridge the gap between research and practice, providing a real-world evaluation of the guidelines.
Implications for practice
I sense that we are running before we can walk by developing these guidelines. The question of what language should and shouldn’t be used to discuss mental health is one that remains to be conclusively answered and I think more work is needed here before we attempt to consolidate this into guidelines. As above, a systematic review combined with more extensive qualitative work would be beneficial here. A much wider priority setting exercise using an approach like the James Lind Alliance’s would also be of benefit to this topic.
Once we have a better understanding of the language deemed acceptable and appropriate by those with lived experience it is of paramount important to continue to work with individuals with experience of mental ill health to work out the best, and most sensitive, way to disseminate this guidance. As somebody with a lived experience of mental ill health myself, I fully appreciate the focus on the language used. However, I sometimes worry that in placing too many rules and restrictions on language we risk undoing the progress we have made in encouraging people to talk openly and honestly about their experiences of mental health. It’s important to me that any language guidelines do not insinuate a judgment or punitive approach to mistakes – but instead aim to educate and inform the public about why certain language might be deemed stigmatising.
Are we trying to run before we can walk? More work needs to be done to figure out what language is deemed acceptable to those with lived experience of mental health, suicide and use of alcohol and other drugs.
Statement of interests
None to disclose.
Links
Primary paper
Paton, E., Jones, E. P., Peprah, J., & Benson, M. (2024). Our Words Matter: Finding Consensus on Evolving and Personal Language Around Suicide, Mental Health Concerns and Alcohol and Other Drug Use. Media International Australia, 1329878X241278005.
Other references
Catchpole, Z. #chatsafe: helping young people communicate safely online about suicide. The Mental Elf, May 2020.
Escandón, K. (2024). Toward non-stigmatizing media and language in mental health: Addressing the social stigma of schizophrenia. Schizophrenia Research, 264, 491-493.
Huggett, C. Language matters: how should we talk about suicide? The Mental Elf, August 2020.
Niederkrotenthaler, T., Braun, M., Pirkis, J., Till, B., Stack, S., Sinyor, M., … & Spittal, M. J. (2020). Association between suicide reporting in the media and suicide: systematic review and meta-analysis. Bmj, 368.
Ross, A. M., Morgan, A. J., Jorm, A. F., & Reavley, N. J. (2019). A systematic review of the impact of media reports of severe mental illness on stigma and discrimination, and interventions that aim to mitigate any adverse impact. Social Psychiatry and Psychiatric Epidemiology, 54, 11-31.



